1. Analysis by Race
American Indians/Alaskan Natives consistently have the highest rate of death. That is followed closely by Whites. That the Total line closely follows the White line is unsurprising given that Whites form the largest racial group. African Americans and Asians fall below the Total line. As we have seen earlier the line for African Americans has risen sharply in the last few years because of sharp increase in drug-related deaths. Asians may have the lowest death rate however, the death rate for Asians continues to rise, not at the accelerated rates of the three groups, but are rising nevertheless.

2. By Race and Gender
I further subdivided the data by gender. In the figure below, females are represented by squares and males by circles.
Every group has shown an increase in deaths from despair, even female Asians who clearly show the lowest rate of increase. As a whole, females show a lower death rate than males. One notable exception is that male Asians have a lower death rate than American Indian/Alaskan Natives and female Whites.
What I find particularly striking about this graph are the lines for American Indian/Alaskan Native Males and White Males. Both lines follow a steeper trajectory with strikingly higher death rates than the other groups. What I find striking as well is that these two lines closely follow each other. And for those two reasons I decided to drill into the data from these two groups with Age as a factor.
3. Analysis of American Indian/Alaskan Native Males and White Males
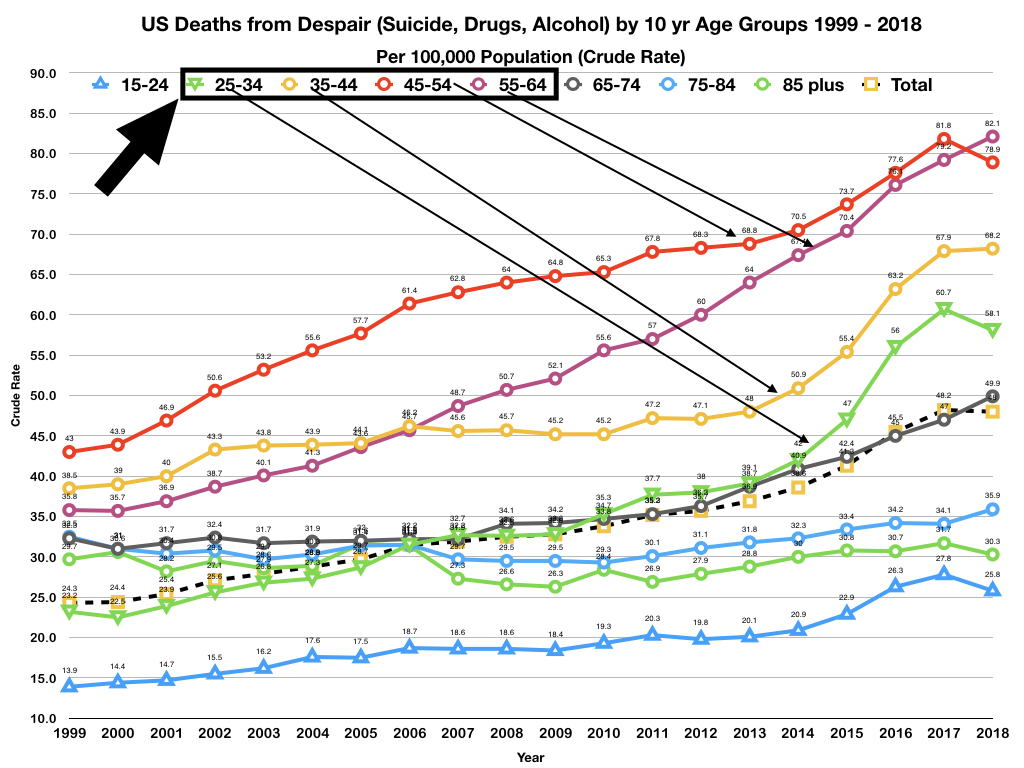
I added age as an analysis factor for these two groups. The figure below shows the results of that analysis.

American Indian/Alaskan Native male lines have downward pointing triangles. White males have circles.
Something to note: American Indians/Alaskan Natives have jagged lines. The reason is that the underlying numbers are relatively small so a relatively small change can seem to show large swings in the crude rate. That being the case one needs to focus not on the swings but on the overall trends that unfortunately point strongly upward.
Something to note: American Indians/Alaskan Natives have jagged lines. The reason is that the underlying numbers are relatively small so a relatively small change can seem to show large swings in the crude rate. That being the case one needs to focus not on the swings but on the overall trends that unfortunately point strongly upward.
I selected most productive years in 10 year age ranges that consist of the 10 year age ranges of:
- 25-34
- 35-44
- 45-54
- 55-64
For both American Indian/Alaskan Native males and White males the most deadly years range from 45 to 64. For American Indian/Alaska Natives males those years have proven particularly deadly, especially in recent years. And it is clear, that for American Indians/Alaskan Native males, deaths from despair begin relatively early in life and become more strongly pronounced as they grow older.
Something that interested me was the American Indian/Alaskan Native and Whites show similar patterns in the 25 to 34 age range.
Two more figures separately show American Indians/Alaskan Native and White males.

 These two groups are clearly at the most risk for death from despair and the numbers are staggeringly high.
These two groups are clearly at the most risk for death from despair and the numbers are staggeringly high.
This series of articles will continue.
Something that interested me was the American Indian/Alaskan Native and Whites show similar patterns in the 25 to 34 age range.
Two more figures separately show American Indians/Alaskan Native and White males.


This series of articles will continue.